
New Survey Finds People With Pulmonary Hypertension Face Serious Health, Social And Financial Impacts
Written by |
Results released Monday, May 5th from Canada’s Pulmonary Hypertension Association (PHA) Patient and Caregiver Survey revealed that those in Canada diagnosed with pulmonary hypertension (PH) are experiencing serious financial, social, and physical burdens as a result of being diagnosed with disease. Chief among the difficulties experienced among the PH patient population is social isolation, lack of education surrounding the disease, and financial and physical burdens — all of which need to be addressed by the medical community and health policy experts.
The poll, which was commissioned by PHA Canada in late 2013, was conducted online by Harris, a leading pollster, and surveyed 179 respondents (118 patients and 61 caregivers). It is the first poll of its kind in Canada that sought to measure the effect that PH has in peoples’ lives, particularly among the – 10,000 Canadians who have been diagnosed with the disease.
[adrotate group=”4″]
“We are grateful to the many Canadians who shared their experiences of living with PH through this important research,” says PHA Canada’s Angie Knott “Their feedback confirms that too many Canadians are still struggling to live and cope with this rare and fatal disease and they have provided us with valuable insights into what changes are needed most across the country to improve lives.”
How PH Leads To Social Isolation, Relationship Issues For Patients and Caregivers
Surprisingly, a plurality of respondents in the poll — more than 70% of patients surveyed and more than 61% of caregivers surveyed — admitted that PH led directly to social isolation and issues in relationships. Most respondents attribute these difficulties to the “invisibility” of PH, according to the survey. Because there is a palpable lack of awareness about the disease, the ignorance lead to misunderstandings among friends, coworkers, and the overall public, all of which leads to a sense of social isolation with patients.
Connect with other patients and share tips on how to manage Pulmonary Hypertension in our forums!
In addition, the physical burden of the disease places many social limitations on those affected by it, with seven in 10 patients surveyed reporting they are unable to play with their children/grandchildren or even help them with their homework. Caregivers are also impacted as those surveyed spend more than half of their time on activities related to caring for their relative with PH.
“Every day has become a challenge since my PH diagnosis,” said Loretta Chu, of Toronto, Ontario, who has lived with PH for eight years. “When you are dealing with symptoms that others cannot visibly see or relate to, people are quick to misunderstand and even judge.”
[adrotate group=”3″]
Physical limitations and reduced quality of life
The PHA Canada Patient and Caregiver Survey also reveals that 85% of patients surveyed experience mild to severe symptoms or limitations with every-day activities such as walking and climbing stairs. More than 40% of patients surveyed report frequently suffering from fatigue, low energy and breathlessness, while another 37% suffer from sleep disorders.
These physical symptoms make it extremely difficult for patients to continue living healthy, happy lives and force many, along with their caregivers, to make dramatic changes to their lifestyle, including their professional and personal relationships. Even with current treatments, one-third of patients surveyed feel there are insufficient medication options to optimally manage their PH.
Opportunity costs — impact on employment and income
Due to the physical limitations of the disease, patients also find it very difficult to maintain their employment, with nearly 60% of those surveyed reporting they are either no longer able to work at all or have partially stopped working due to their PH. There is a similar impact on caregivers too, with close to 40%* of caregivers forced to make employment changes to care for someone with PH.
This inability to work carries enormous psychological and social challenges, and also has a tremendous impact on the financial stability of those affected by PH, many of whom are in their prime earning years. Of those surveyed, nearly 90% of patients say that their income has decreased by more than 25% due to their PH-induced change in employment, with nearly half saying their income has reduced by 50% or more.
“The symptoms of PH, like chronic fatigue and shortness of breath, make it extremely difficult to carry out every-day activities that most Canadians take for granted,” said Loretta Chu, who also leads a support group for PH patients in Toronto. “This obviously makes it very hard to maintain one’s employment which brings not only financial income and stability but also a sense of purpose, achievement and social interaction. When all of this is taken from someone, the burden is tremendous.”
The killer waiting game — delays in proper diagnosis
Citing several reasons, including a lack of recognition of symptoms among patients and their primary healthcare providers, the PHA Canada Patient and Caregiver Survey reveals that surveyed patients waited an average of three years for proper diagnosis. While more than half of patients surveyed state that their family doctor did not initially recognize the symptoms of PH and refer them to the proper specialist, patients themselves suffered an average of 31 and 44 months with breathlessness/dyspnea and tiredness/fatigue respectively before even seeking medical attention.
“This survey has uncovered an alarming lack of awareness of PH and its symptoms. Like many rare and fatal diseases, early diagnosis and access to effective treatment can make an enormous impact on outcomes and quality of life. We now know that we must do a better job of educating both doctors and the general public in PH to help improve, and save lives,” says Pulmonary Hypertension Association of CanadaChair Dr. Sanjay Mehta
Harris Poll conducted the online Burden of Illness survey across Canada on behalf of PHA Canada between September 12 and October 25, 2013, among a total of 179 respondents (118 patients and 61 caregivers). Statistical comparisons were conducted at the 95% level of confidence between groups where base sizes allowed. The average age of the patients and caregivers who completed the survey was 51 and 47 respectively. Respondents completed online questionnaires developed by PHA Canada with the guidance of a steering committee including PH doctors, nurses, patients and caregivers. The survey was conducted by Harris Interactive and funded by Actelion Pharmaceuticals Canada Inc. through an unrestricted educational grant to PHA Canada. It is the first survey conducted in Canada to measure the impact of PH on patients and their caregivers, and has allowed a deeper understanding of PH and the physical, psychological and emotional burden the disease has on the lives of those affected by it.
The Pulmonary Hypertension Association of Canada (PHA Canada) is a national, registered charity working to end the invisibility and isolation often experienced by those living with this life-changing disease. To learn more about PHA Canada and pulmonary hypertension, visit:
https://www.PHACanada.ca
In the U.S. the Pulmonary Hypertension Association a young organization that is changing the history of an illness. From simple beginnings — four women who met around a kitchen table in Florida in 1990 – the PHA has evolved into a community of well over 10,000 pulmonary hypertension patients, caregivers, family members and medical professionals. Beginning in 1999, the PHA held golf tournaments in Houston and Dallas to continue to foster public awareness of PH, support research and sustain its growing programs. Instrumental advocacy efforts in Congress heightened PH awareness as well. Representative Kevin Brady (R-TX), motivated by his personal connections with several PH patients in his district, introduced the first PH-specific bill in Congress in 2000. Several years later, the late Representative Tom Lantos (D-CA) joined Representative Brady in introducing a new PH bill. These efforts pushed PHA toward closer relationships with Members of Congress, intensifying support for PH legislation. The PHA raised over $130,000 in 1990, and awareness of PH surged.
Today the PHA is a 501(c)(3) nonprofit organization. What started as a small support group at a kitchen table became a dynamic organization composed of over 13,000 members and supporters only 20 years later. In 2011, the PHA annual budget increased to over $10 million. PHA’s original one-page newsletter, Pathlight, grew to a 55-page quarterly publication. The PHA has worked closely with more than 50 PH associations around the world, and earned Charity Navigator’s four-star rating eight years in a row, the highest recognition conferred by the leading charity evaluator in America. The organization continues to work toward ending isolation, provide education, involve its constituents in everything it does, and ultimately top find a cure for pulmonary hypertension.
Twenty years ago there were no pulmonary hypertension treatments available. Through focused research there are now twelve PH-specific treatments with more in development. In just a little under a decade, PHA’s Research Program has committed more than $12.5 million for PH research by leveraging partnerships with the National Heart, Lung, and Blood Institute (NHLBI) and the American Thoracic Society (ATS). The organization has supported over 49 promising researchers through four independently reviewed, cutting-edge research programs.
For more information, visit:
https://www.phassociation.org/
Another U.S. PH support organization, PHCentral, began in 1997 as a Website, and over the years has developed into a well-respected PH resource for individuals and families seeking information, friendship and support. Because PHCentral remains an all-volunteer staff, the pioneer spirit has not been lost. In the summer of 2009, PHCentral launched a new, friendlier website to continue work in the PH Community, adding new sections and expanding old ones, and now has volunteers from Australia, Canada, and Germany, as well as America. For more information, visit:
https://www.phcentral.org/
[adrotate group=”3″]
Pulmonary Hypertension: What You Need To Know
While most people have heard of asthma, diabetes, and cardiovascular disease, few are aware of pulmonary hypertension (PH), a devastating, life-threatening condition that literally takes a person’s breath away. Even fewer know about chronic thromboembolic pulmonary hypertension (CTEPH), which is a type of PH.
Pulmonary Hypertension (PH) is a progressive life-threatening condition characterized by high blood pressure in the arteries of the lungs. Idiopathic PAH (IPAH) has an annual incidence of 1-2 cases per million people in the US and Europe and is 2-4 times as common in women as in men. According to PAH-info.com, it is estimated around 5,000 Canadians have been diagnosed with PH, but as many as 10,000 may be affected by the condition. The mean age at diagnosis is around 45 years, although the onset of symptoms can occur at any age. Of those diagnosed with PH, a small subgroup will be diagnosed with chronic thromboembolic pulmonary hypertension (CTEPH). CTEPH can potentially be corrected by surgery.
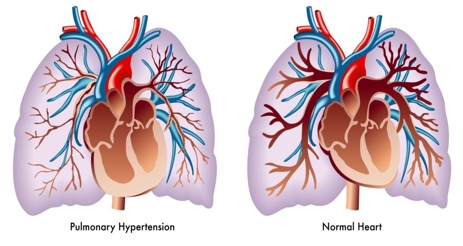
Pulmonary hypertension (or PH), first identified by Ernst von Romberg in 1891, affects the arteries of the lungs, which become narrowed and scarred in people with the disease. This can result in almost complete closing of the arteries, which can in turn lead to heart failure. PH symptoms include shortness of breath; bluish hands, feet and lips; swelling of hands and feet; light-headedness and dizziness; chest pain; exhaustion and fainting. Because it shares many symptoms with other diseases, PH — a terminal disease for which there is currently no cure — is often misdiagnosed. Pulmonary hypertension is more common among women, non-Hispanic blacks, and among people aged 75 or older.
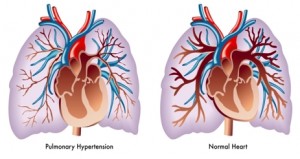
The U.S. National Library of Medicine (NLM) describes pulmonary hypertension as abnormally high blood pressure in the arteries of the lungs that makes the right side of the heart work harder than normal. The right side of the heart pumps blood through the lungs, where it picks up oxygen. Blood returns to the left side of the heart, where it is pumped to the rest of the body. When the small arteries (blood vessels) of the lung become narrowed, they cannot carry as much blood. When this happens, pressure builds up — which is called pulmonary hypertension. The heart needs to work harder to force blood through the vessels against this pressure, and over time, this causes the right side of the heart to become larger. Ultimately, heart failure affects the right side of the heart. This is called cor pulmonale.
The NLM says pulmonary hypertension may be caused by autoimmune diseases that damage the lungs, such as scleroderma and rheumatoid arthritis, birth defects of the heart, blood clots in the lung (pulmonary embolism), heart failure, heart valve disease, HIV infection, low oxygen levels in the blood for a long time (chronic), lung disease, such as COPD or pulmonary fibrosis, medicines (for example, certain diet drugs), and obstructive sleep apnea, but in many patients, the cause of pulmonary hypertension is unknown. In that case, the condition is called idiopathic pulmonary arterial hypertension (IPAH). IPAH is rare, and affects more women than men. If pulmonary hypertension is caused by a known medicine or medical condition, it is called secondary pulmonary hypertension.
 “Patients with PH and CTEPH most commonly suffer from progressive shortness of breath or dyspnea, which can become disabling. Because dyspnea can also be due to many other less severe diseases of the heart and lungs as well as being unfit, there is often a 2-3 year delay in the diagnosis of PH,” says Dr. Sanjay Mehta MD, FRCPC, FCCP, Professor of Medicine and Director Southwest Ontario PH Clinic in London, Ontario and Chair, Board of Directors, PHA Canada. “This is a serious issue in the care of PH patients, as early diagnosis of PH can mean the difference between life and death. It is PHA Canada’s priority to increase awareness of PH and especially CTEPH, in order to promote earlier diagnosis and excellent medical care of PH patients, leading to a better quality of life and longer survival.”
“Patients with PH and CTEPH most commonly suffer from progressive shortness of breath or dyspnea, which can become disabling. Because dyspnea can also be due to many other less severe diseases of the heart and lungs as well as being unfit, there is often a 2-3 year delay in the diagnosis of PH,” says Dr. Sanjay Mehta MD, FRCPC, FCCP, Professor of Medicine and Director Southwest Ontario PH Clinic in London, Ontario and Chair, Board of Directors, PHA Canada. “This is a serious issue in the care of PH patients, as early diagnosis of PH can mean the difference between life and death. It is PHA Canada’s priority to increase awareness of PH and especially CTEPH, in order to promote earlier diagnosis and excellent medical care of PH patients, leading to a better quality of life and longer survival.”
Dr. Mehta, is additionally Chair of Medical Advisory Committee to PHA Canada, Professor of Medicine at the University of Western Ontario, and Director of the Southwest Ontario Pulmonary Hypertension Clinic at the London Health Sciences Center in London, Canada. He is also Chair of the Pulmonary Vascular Disease Committee of the Canadian Thoracic Society. Dr. Mehta has been caring for patients with PH and doing research in PH since 1989. Current PH activities include the direct clinical care of PH patients, research studies using new medications and new methods to assess PH patients, further developing the LivingwithPH.ca website for education of Canada PH patients/caregivers, and developing the first PH clinical practice guidelines for Canada. Dr. Mehta has been a member of the Board of Directors and Medical Advisory to PHA Canada since 2008, and the PHA Canada Board Chair since September 2013.
New Social Media Campaign Promotes Awareness of This Frequently Misdiagnosed Form of Lung Disease
The Pulmonary Hypertension Association of Canada (PHA Canada) has launched a new social media awareness campaign with the objective of promoting greater awareness of pulmonary hypertension (PH), in order to promote earlier diagnosis.”Invisibility” of the disease, delays in diagnosis and physical, social and financial burdens among top challenges to be addressed.
Key cornerstones of the PHA Canada campaign include new CTEPH-focused pages on the PHA Canada website and a unique Twitter handle– @CTEPHAware — dedicated specifically to CTEPH. The goal is to bring CTEPH to life through these educational platforms using ‘real-life’ story telling through video vignettes and shorter 6-second video clips (see video clip links at the end of this article).
“If a picture is worth a thousand words, we’re hoping compelling video vignettes will take our message to new heights,” says Angie Knott, National Manager, PHA Canada. “Our goal is to educate Canadians about CTEPH in a way that really helps them understand and learn. We are thrilled to offer new platforms of support and education to the PH community, including people at risk of developing PH and CTEPH and their caregivers.”
Notes:
1) Mehta, S et al Diagnostic evaluation and management of chronic thromboembolic pulmonary hypertension: A clinical practice guideline. Can Respir J 2010; 17(6):301-334.
2) PHA Canada website, What is PH? https://www.phacanada.ca/en/education/
3) PHA Canada website, What is PH? https://www.phacanada.ca/en/education/ Last accessed February 5, 2014
Video resources:
Video with caption: “Video: Lynda is a CTEPH patient who was diagnosed in 2011. This is her CTEPH story.”. Video available at: https://www.youtube.com/watch?v=CE1LcsXi1hE
Video with caption: “Video: Dianne is a CTEPH patient who was diagnosed in 2013. This is her CTEPH story.”. Video available at: https://www.youtube.com/watch?v=tsK3U2caj40
Video with caption: “Dr. Sanjay Mehta is a CTEPH-treating doctor.”. Video available at: https://www.youtube.com/watch?v=TgVlfXXpjTo
For more information, (Centers for Disease Control and Prevention) visit:
https://goo.gl/QnEsbV
Sources:
Pulmonary Hypertension Association of Canada
Pulmonary Hypertension Association (U.S.)
PHCentral
Centers for Disease Control and Prevention
The U.S. National Library of Medicine (NLM)
PAH-info.com
Wikipedia
Image Credits:
Pulmonary Hypertension Association of Canada
[adrotate group=”3″]




Shawna Wonderling Rupple
I agree the general public needs to be educated but so do medical professionals who care for you who are other than your pulmonologist (primary care physicians, er doctors, etc...)
ann b wall
I saw 5 doctors that didn't diagnose me-pulmonologists and one cardiologist. My brother's doctor recommended Dr H Palevsky at U of Penn ,a certified PH program. I am a lucky miracle. thanks to Dr Palevsky and the staff at Harron Lung center.
Lorraine Ortiz
My role has taken a 360 degree turn, as I am now a caregiver and not a partner in life. this PAH is a life changer. It has affected us, not only physically, but, emotionally, socially, and financially. My partner was told that if he did not try this Veletri infusion, he would probably only have one year to live. And, as I look at him, he looks so fragile and debillitated. Was this even worth it?