
American Heart Association Publishes Major Update on Pulmonary Hypertension Advances
Written by |
In a recent review published in Circulation, the official Journal of the American Heart Association, Jonathan and Stuart Rich examined the current status of the epidemiology, prognosis, and update of the clinical classification for PH. In the review, the authors mainly focus on the diagnostic approach of suspected Pulmonary Hypertension (PH), emphasizing the key features that a clinician needs to consider. Moreover, the authors reviewed an evolving conceptual framework for viewing the pulmonary vasculature and the right ventricle as a single, coupled cardiopulmonary unit.
In terms of epidemiology and prognosis, the AHA notes that PH prevalence remains unknown, with an estimation that 83% of patients with heart failure have PH. PH is considered to be a disease with multifactorial etiology. In terms of classification, PH diagnoses can fall into 5 distinct groups: PAH (Group 1); PH secondary to left heart disease (Group 2); PH secondary to lung disease (Group 3); chronic thromboembolic PH (Group 4); and PH secondary to unclear or multifactorial mechanisms (Group 5).
[adrotate group=”4″]
With regards to clinical assessment of the patient with suspected PH, the AHA believes that clinicians should first look at symptom history, which usually includes dyspnea with exertion, the onset of right ventricular failure, lower extremity edema or complaints of abdominal distention, or early satiety secondary to venous congestion — all of which are characteristic symptoms of the disease. Moreover, symptoms such as angina reflecting demand ischemia from impaired coronary blood flow to a markedly hypertrophied right ventricle (RVH) are also a consideration. As cardiac output becomes fixed and eventually falls, patients may have episodes of syncope or near-syncope, an ominous symptom requiring prompt medical attention. There are patients with PH related to left ventricular dysfunction that can show orthopnea or paroxysmal nocturnal dyspnea. Hemoptysis is uncommon but can also occur.
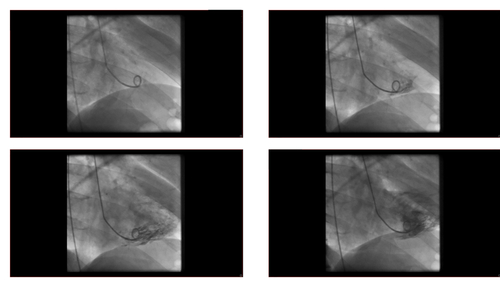
Secondly, if an Echocardiography is not compatible with PH, the authors mention that the clinician should consider other causes for the symptoms or recheck the patient. If the Echocardiography is compatible with PH, other common causes such as heart disease and lung cancer should be examined, and a careful consideration should be given to the history, signs, and risk factors associated with the disease, as well as result from ECG, X-Ray, PFT including DLCO, BGA, and HR-CT. If heart disease and lung cancer are positive, the clinician should treat the underlying disease if no signs of severe PH/RV are present. If there are signs of severe PH/RV dysfunction, the clinician should refer the patient to a PH expert. If no diagnoses of a secondary disease are present, V/Q scintigraphy should be performed. If there are unmatched perfusion defects, clinicians should consider that CTPH is likely (CT angiography, RHC plus PA) and refer the patient to a PEA expert. If not, the next procedure should be to conduct an RHC. Other causes may be present if there is no PAPm >25mmHg, PAWP <15mmHg, and PVR<3WU. However, if these features are present, the patient is likely to have PAH, and specified diagnostic tests should confirm the disease, such as CTD, Drugs Toxins, HIV, PVOD PCH, CHO, Porto-Pulmonary, Schistosomiaisis and Idiopathic or Heritable PAH.
[adrotate group=”3″]
What AHA adds to the knowledge of PH diagnosis in this review is the crucial clinical evaluation of the status of both the pulmonary vasculature and the right ventricle, and that such characterizations should ideally be made and considered as an integrated cardiopulmonary unit.
The AHA believes that PAH the RV have traditionally been difficult to study because of their unique geometry and the lack of simple, reliable, and quantifiable noninvasive assessments. However, the emergence of CMR and other innovative modalities such as PET and measurements of ventriculoarterial coupling are encouraging developments to more comprehensively assess and follow RV function. Yet, the authors note that these are costly methods and are not always available outside of specialized centers. The AHA reports that a careful and detailed physical examination will continue to provide the clinician with useful information about the severity and response to therapy in most patients.


Leave a comment
Fill in the required fields to post. Your email address will not be published.